Kidneys pathology. (Subject 17) презентация
Содержание
- 2. Lecture Plan
- 3. The kidneys are essentially regulatory organs which maintain the volume and
- 4. Homeostasis: Homeostasis: Sodium/Volume; Water/Osmolarity; Asid/Base; Electrolytes (K+, Ca++, Mg++, HPO4)
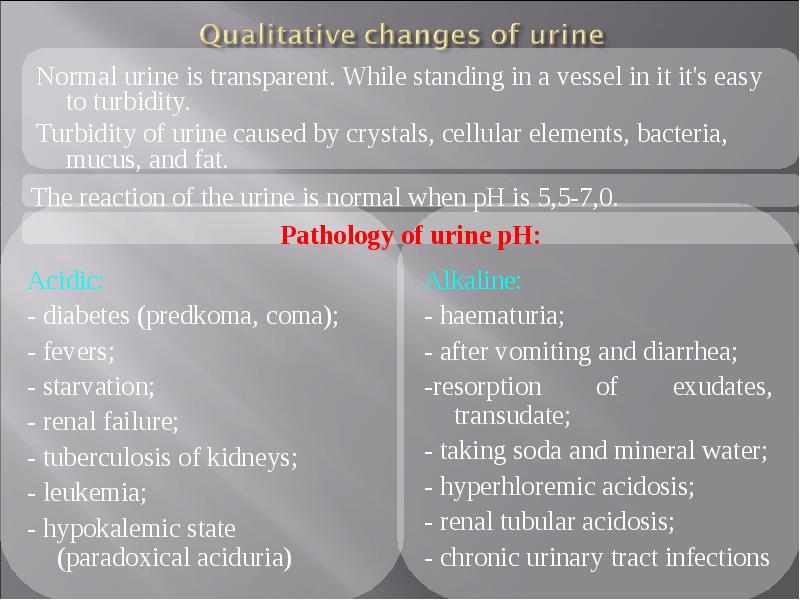
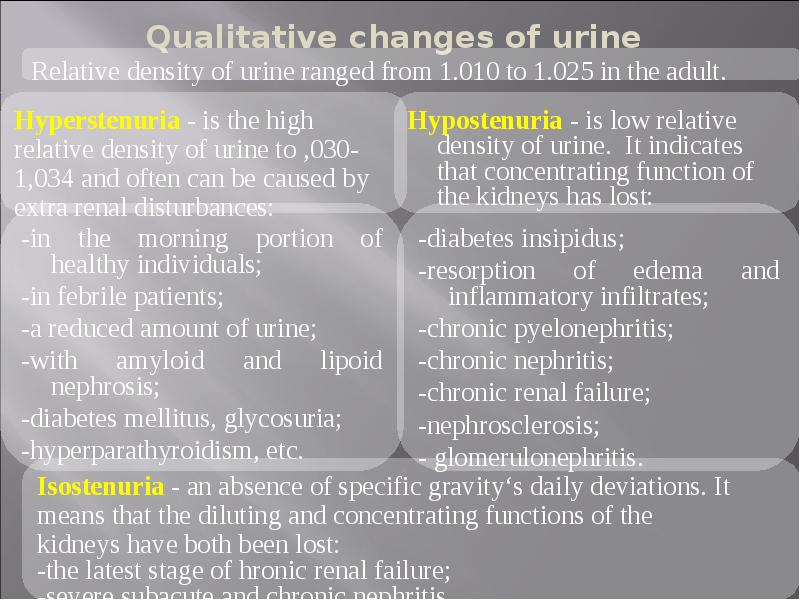
- 5. Normal urine volume is 750 to 2000 ml per day.
- 6. Hypohromuriya is physiological if it’s caused by polyuria as a result
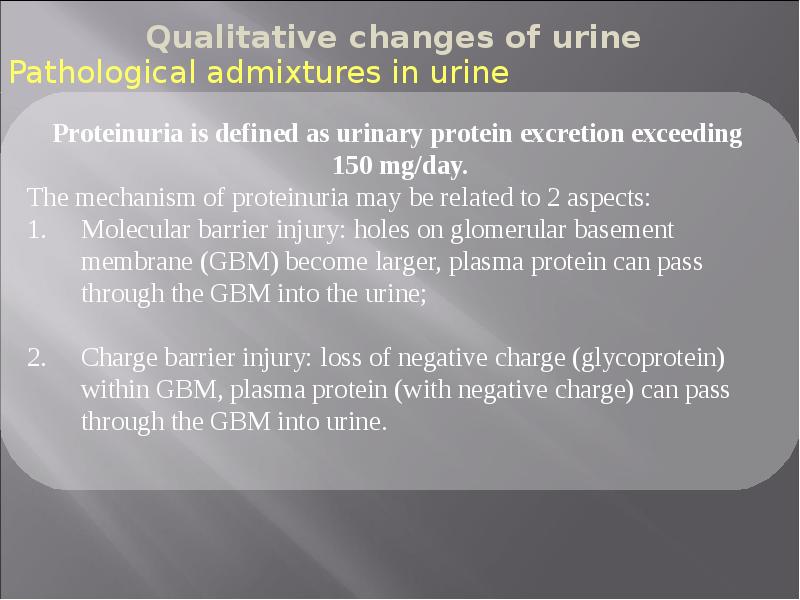
- 10. Nonpathological proteinuria - excessive protein excretion is apparently not the result
- 11. Haematuria is defined as appearance of RBC in urine Haematuria
- 12. Visible (macroscopic) haematuria (VH) Visible (macroscopic) haematuria (VH) Non-visible (microscopic) haematuria
- 17. Clinical: Clinical: 1. Primary - are caused by kidney pathology (acute
- 18. In each of the clinical entities with glomerular proliferation, the inflammation
- 19. APSGN is primarily a disease of school-age children (5 - 15
- 21. Nephritic Syndrome - is the acute onset of: Nephritic Syndrome -
- 22. Nephrotic syndrome - is a group of diseases having different pathogenesis
- 23. I. Primary Glomerulonephritis: I. Primary Glomerulonephritis: Minimal change disease (most common
- 25. Renal failure often refers to significant loss of renal function.
- 26. Acute renal failure commonly is classified as: Acute renal failure commonly
- 28. Pathophysiology and Clinical manifestations of Uremic syndrome Pathophysiology and Clinical manifestations
- 29. Retention of nitrogenous wastes Retention of nitrogenous wastes Increased intracellular Na+
- 30. 1. Skin manifestations - pruritus, uremic "frost", skin 1. Skin
- 32. Thank you for your attention Thank you for your attention
- 33. Скачать презентацию


")




 haematuria (VH)
Visible (macroscopic) haematuria (VH)
Non-visible (microscopic) haematuria")












Слайды и текст этой презентации
Слайд 1
Описание слайда:
Слайд 2
Описание слайда:
Lecture Plan
Слайд 3
Описание слайда:
The kidneys are essentially regulatory organs which maintain the volume and composition of body fluid by filtration of the blood and selective reabsorption or secretion of filtered solutes.
The kidneys are essentially regulatory organs which maintain the volume and composition of body fluid by filtration of the blood and selective reabsorption or secretion of filtered solutes.
The kidneys take their blood supply directly from the aorta via the renal arteries; blood is returned to the inferior vena cava via the renal veins
The kidneys are critical in regulating the internal environment of the body.
Слайд 4
Описание слайда:
Homeostasis:
Homeostasis:
Sodium/Volume;
Water/Osmolarity;
Asid/Base;
Electrolytes (K+, Ca++, Mg++, HPO4)
Слайд 5
Описание слайда:
Normal urine volume is 750 to 2000 ml per day.
Normal urine volume is 750 to 2000 ml per day.
Слайд 6
Описание слайда:
Hypohromuriya is physiological if it’s caused by polyuria as a result of increased drinking, diuretics food.
Hypohromuriya is physiological if it’s caused by polyuria as a result of increased drinking, diuretics food.
Pathological hypohromuriya is developed due to:
- diabetes;
- diabetes insipidus;
- nephrosclerosis.
Слайд 7
Описание слайда:
Слайд 8
Описание слайда:
Слайд 9
Описание слайда:
Слайд 10
Описание слайда:
Nonpathological proteinuria - excessive protein excretion is apparently not the result of a disease. The level of proteinuria is generally less than 1 g/day and is never associated with edema.
Nonpathological proteinuria - excessive protein excretion is apparently not the result of a disease. The level of proteinuria is generally less than 1 g/day and is never associated with edema.
Postural (orthostatic)
Febrile
Exercise-induced
Pathological proteinuria results from glomerular or tubular disorders. It is characterized by persistent and severe intensity - more than 3.5 g/l.
Tubular:
Inherited - Cystinosis, Wilson disease, Lowe syndrome);
Acquired - Antibiotic-induced, Interstitial nephritis, Acute tubular necrosis, Heavy metal poisoning);
Glomerular - nephrotic syndrome, idiopathic, mesangial proliferation, focal sclerosis, glomerulonephritis, systemic diseases (lupus erythematosus), drugs, hypertension, diabetes mellitus, hemolytic uremic syndrome and other renal diseases.
Слайд 11
Описание слайда:
Haematuria is defined as appearance of RBC in urine
Haematuria is defined as appearance of RBC in urine
Common Causes of Glomerular Hematuria:
IgA nephropathy (Berger’s disease);
Thin glomerular basement membrane disease;
Hereditary nephritis (Alport’s syndrome).
Common Causes of Non-Glomerular Hematuria:
Upper Tract:
Urolithiasis;
Pyelonephritis;
Renal cell cancer;
Transitional cell carcinoma;
Urinary obstruction;
Benign hematuria
Lower Tract:
Bacterial cystitis;
Benign prostatic hyperplasia;
Transitional cell carcinoma;
Strenuous exercise (“marathon runner’s hematuria”);
Spurious hematuria (e.g. menses);
Instrumentation;
Benign hematuria
Слайд 12
Описание слайда:
Visible (macroscopic) haematuria (VH)
Visible (macroscopic) haematuria (VH)
Non-visible (microscopic) haematuria (NVH) - is not visible to the naked eye.
Macroscopic hematuria can be divided into three types:
Initial Hematuria - bleeding that occurs at the start of urination. This could indicate a problem in the urethra in women or the prostate (in men).
Total Hematuria - bleeding that occurs while urinating is known as total hematuria. Men could experience total hematuria because of an enlarged prostrate. In women, vaginal bleeding during urination could be an indication of an infection in the bladder, ureter or kidneys.
Terminal Hematuria - bleeding after urination in men and women. Blood after urination in women is usually indicative of a bladder infection. Men can also experience terminal hematuria because of prostate diseases.
Слайд 13
Описание слайда:
Слайд 14
Описание слайда:
Слайд 15
Описание слайда:
Слайд 16
Описание слайда:
Слайд 17
Описание слайда:
Clinical:
Clinical:
1. Primary - are caused by kidney pathology (acute diffuse proliferative postinfectious GN, membranoproliferative GN, rapid progressive GN, lipoid nephrosis, focal segmental sclerosis, membranous glomerulopathy, IgA nephropathy, chronic glomerulonephritis);
2. Secondary - are caused by other organs and systems pathology or systemic diseases: (SLE, diabetes mellitus, amyloidosis, Henoch-Schenlein purpura, bacterial endocarditis);
3. Hereditary disorders - Alport syndrome, thin membrane disease etc.
Histopathological (patterns established on light microscopy):
Proliferative and nonproliferative variants are possible.
Membranous;
Mesangiocapillary;
Focal segmental glomerulosclerosis etc.
Etiological:
Inflammatory - the dominant aetiological agent for GN are bacteria, viruses, parasites;
Noninflammatory – immunopathological;
Idiopathic.
Слайд 18
Описание слайда:
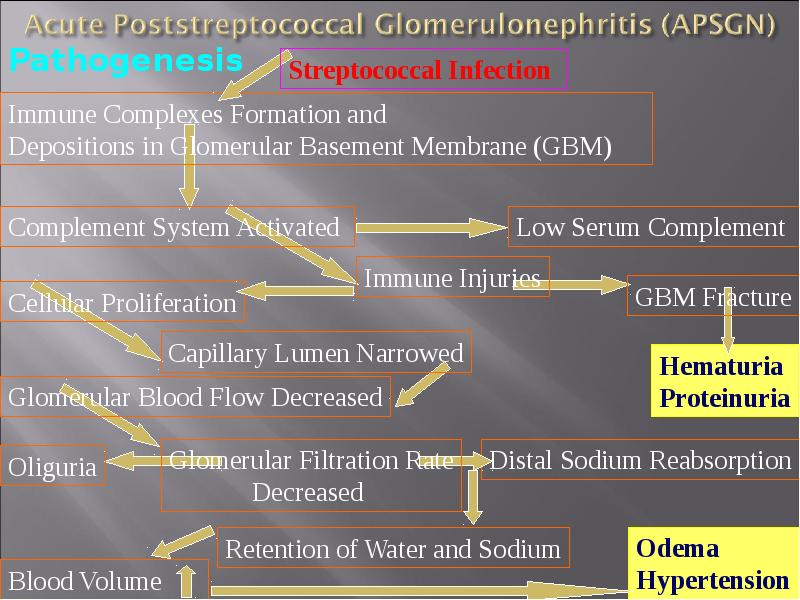
In each of the clinical entities with glomerular proliferation, the inflammation process leads to:
In each of the clinical entities with glomerular proliferation, the inflammation process leads to:
- decreased glomerular perfusion,
- retention of salt and water
- potential development of hypertension and edema.
Acute Poststreptococcal Glomerulonephritis (APSGN):
- is clearly the most frequent form of acute postinfectious glomerulonephritis;
- the clinical syndrome is often regarded as the prototype of the acute nephritic syndrome;
- Group A I²-hemolytic streptococcus serologic testing confirms recent infection (pharyngitis or pyoderma).
Слайд 19
Описание слайда:
APSGN is primarily a disease of school-age children (5 - 15 years) and is more common in boys.
APSGN is primarily a disease of school-age children (5 - 15 years) and is more common in boys.
Patients are usually afebrile with a latency period following pharyngitis of 1 to 2 weeks and 3 to 6 weeks after a skin infection.
The most common presenting features are edema and gross hematuria. Essentially all the patients have microhematuria. The urine often has a color, described as smoky, cola-colored, or tea-colored.
Hypertension is common but is usually mild to moderate; rarely, hypertensive encephalopathy has been reported.
Nephritic syndrome is a typical manifestation of APSGN.
Fewer than 5% of patients develop nephrotic syndrome with significant proteinuria and a slightly depressed serum albumin level.
Слайд 20
Описание слайда:
Слайд 21
Описание слайда:
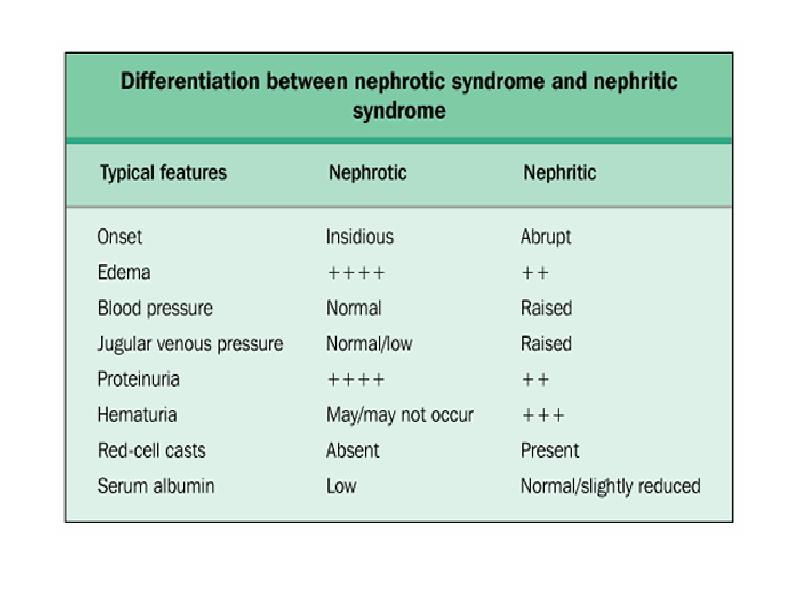
Nephritic Syndrome - is the acute onset of:
Nephritic Syndrome - is the acute onset of:
Hematuria - may be microscopic or macroscopic. Podocytes develop large pores which allow blood and protein through.
Proteinuria - small amount, < 3.5 g/24 hr).
Hypertension is generally mild.
Oedema is usually mild and results from sodium and water retention.
Oliguria (low urine volume <300ml/day due to renal function been poor).
Red cell casts
Causes of Acute Nephritis:
I. Primary Glomerulonephritis - acute GN (post-streptococcal, non-streptococcal, rapidly progressive GN, membrano-proliferative GN, focal GN, IgA nephropathy).
II. Systemic Disease (SLE, polyarteritis nodosa, Wegener's granulomatosis, Henoch-Schonlein purpura, cryoglobulinaemia).
Слайд 22
Описание слайда:
Nephrotic syndrome - is a group of diseases having different pathogenesis and characterized by clinical findings of:
Nephrotic syndrome - is a group of diseases having different pathogenesis and characterized by clinical findings of:
Massive proteinuria (>3.5g in 24hrs, urine looks frothy), mostly consists of loss of albumin.
Hypoalbuminemia (albumin is lost in the urine due to gaps in podocytes allowing proteins to escape).
Oedema - is usually peripheral (swelling around ankles & eyes) due to:
loss of albumin and intravascular oncotic pressure decreasing;
sodium and water retention (secondary hyperaldosteronism, but osmotic pressure of blood is decreased);
increase of hydrodynamic intravascular pressure and vessels permobility (fluid moves out of vessels);
Hyperlipidemia/hyperlipiduria is caused by:
Hypoproteinemia stimulates protein synthesis in the liver, resulting in the overproduction of lipoproteins;
Lipid catabolism is decreased due to lower levels of lipoprotein lipase.
Hyperlipiduria is due to hyperlipidemia.
Слайд 23
Описание слайда:
I. Primary Glomerulonephritis:
I. Primary Glomerulonephritis:
Minimal change disease (most common in children);
Membranous GN (most common in adults);
Membranoproliferative GN;
Focal GN;
IgA Nephropathy
II. Systemic Disease (diabetes mellitus, amyloidosis, SLE)
III. Systemic Infections:
Viral infections (HBV, HCV, HIV);
Bacterial infections (Bacterial endocarditis, syphilis, leprosy);
Protozoa and parasites (P. falciparum malaria, filariasis)
IV. Hypersensitivity Reactions:
Drugs (penicillamine, tolbutamide, heroin addiction);
Bee stings, snake bite, poison ivy
V. Malignancy (carcinomas, myeloma, Hodgkin's disease)
VI. Pregnancy (toxaemia of pregnancy)
VII Circulator Disturbances (renal vein thrombosis, constrictive pericarditis)
VIII. Hereditary Disease (Alport's disease, nail-patella syndrome)
Слайд 24
Описание слайда:
Слайд 25
Описание слайда:
Renal failure often refers to significant loss of renal function.
Renal failure often refers to significant loss of renal function.
When less than 10% of renal function remains, this is termed end-stage renal failure (ESRF).
Renal failure may be:
- acute as usual is reversible process;
- chronic is termed end-stage renal failure (ESRF).
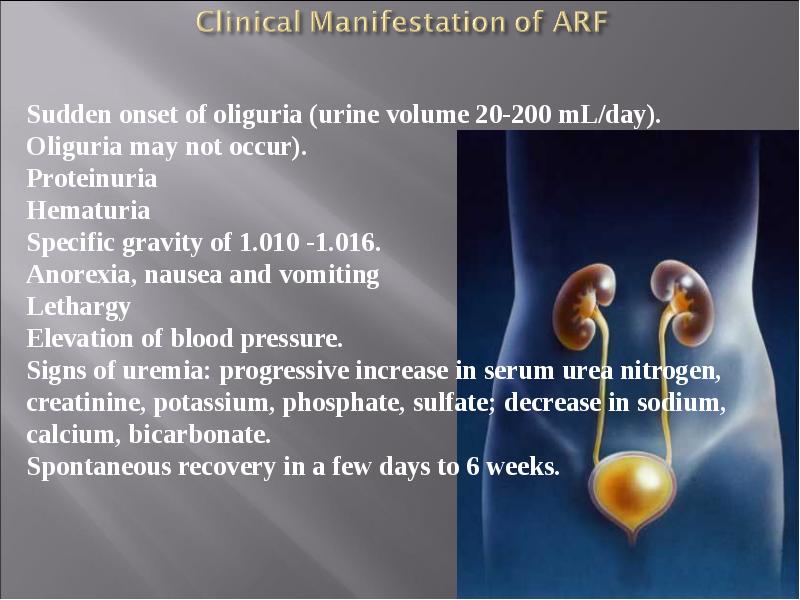
Acute renal failure (ARF) is an abrupt reduction in renal function with elevation of Blood Urea Nitrogen (BUN) and plasma creatinine levels, usually associated with oliguria (urine output of less than 30 ml/hr or less than 400 ml/day), although urine output may be normal or increased.
Слайд 26
Описание слайда:
Acute renal failure commonly is classified as:
Acute renal failure commonly is classified as:
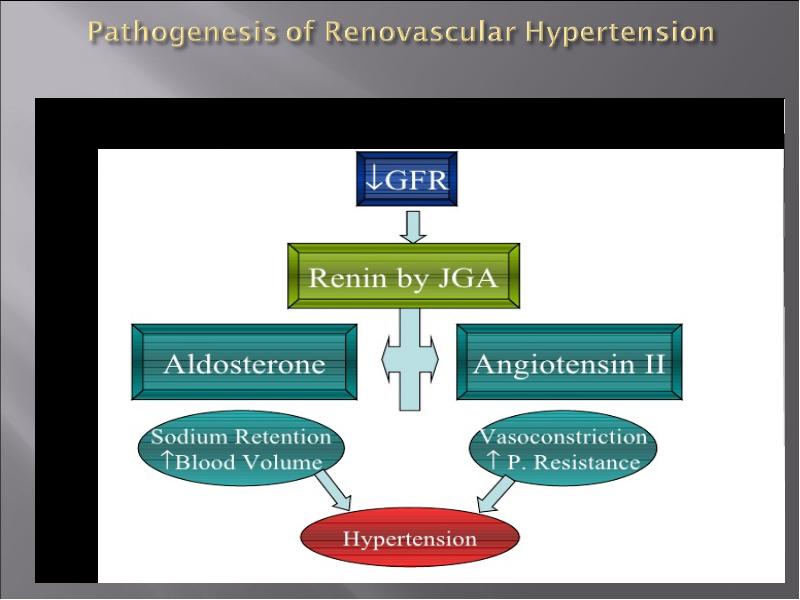
Pre-renal - is caused by impaired renal blood flow.
The GFR declines because of the decrease in filtration
pressure. Poor perfusion can result from hypotension,
renal vasoconstriction,, hypovolemia, hemorrhage,
or inadequate cardiac output.
Intra-renal - may result from pre-renal acute renal
failure (e.g., acute tubular necrosis or cortical necrosis)
or many other diseases, including acute glomerulonephritis,
malignant hypertension, disseminated intravascular
coagulation, and renal vasculitis.
Post-renal - usually occurs with bilaterally urinary tract
obstruction (e.g., bladder outlet obstruction,
prostatic hypertrophy, or bilateral ureteral
obstruction). Several hours of anuria with flank
pain followed by polyuria is a characteristic
finding. This type of renal failure can occur
after diagnostic catheterization of the ureters.
Слайд 27
Описание слайда:
Слайд 28
Описание слайда:
Pathophysiology and Clinical manifestations of Uremic syndrome
Pathophysiology and Clinical manifestations of Uremic syndrome
Uremia is a syndrome of renal failure and includes elevated blood urea and creatinine levels accompanied by fatigue, anorexia, nausea, vomiting, pruritus, and neurologic changes. Usually develops when the creatinine clearance falls to less than 10 mL/min.
Azotemia means increased serum urea levels and frequently increased creatinine levels as well. Renal failure causes azotemia.
Both azotemia and uremia indicate an accumulation of nitrogenous waste products in the blood.
Слайд 29
Описание слайда:
Retention of nitrogenous wastes
Retention of nitrogenous wastes
Increased intracellular Na+ and water
Decreased intracellular K+
Increased levels of bioactive substances normally cleared renally (hormones)
Decreased levels of hormones and other mediators prodesed by the kidney
Decrease basal body temperature
Diminished lipoprotein lipase activity
Слайд 30
Описание слайда:
1. Skin manifestations - pruritus, uremic "frost", skin
1. Skin manifestations - pruritus, uremic "frost", skin
2. Cardiac manifestations - uremic pericarditis
3. Neurological manifestations - peripheral neuropathy
4. Pulmonary complications - pneumonitis and hemorrhage
5. Hematopoietic manifestations - anemia, bleeding diathesis
6. Skeletal abnormalities - renal osteodystrophy (secondary hyperparathyroidism)
7. Other metabolic imbalances
Слайд 31
Описание слайда:
Слайд 32
Описание слайда:
Thank you for your attention
Thank you for your attention
Скачать презентацию на тему Kidneys pathology. (Subject 17) можно ниже: