ENDOMETRIOSIS презентация
Содержание
- 2. ENDOMETRIOSIS INTRODUCTION OF ENDOMETRIOSIS SITES AETIOLOGY THEORIES FOR ENDOMETRIOSIS CLINICAL FEATURES
- 4. INTRODUCTION Endometriosis initially described by Von Rokitansky in 1860 Endometriosis
- 5. SITES ABDOMINAL Most common site -
- 7. EXTRA-ABDOMINAL EXTRA-ABDOMINAL Common sites - Abdominal scar
- 9. AETIOLOGY Age - 30-40 years(most common) - between the menarche and
- 10. Theories for Endometriosis Retrograde menstruation (Sampson’s theory) Metaplasia of coelomic epithelium
- 11. Retrograde menstruation ( Samson’s Theory) John Sampson first postulated that endometriosis
- 13. Coelemic metaplasia( Mayer And Ivanol) In this theory, the germinal epithelia
- 14. Lymphatic Theory (vascular theory ) Endometrial cell can be transported to
- 15. Genetic factors The risk or endometriosis is 7 times greater if
- 16. Autoimmune theory In cellular immunity, can facilitate the successful implantation
- 17. Induction theory The induction theory is, in principle, an extension
- 18. Inflamation Substantial evidence suggests that endometriosis is associated with a
- 19. Pathophysiology Endometriosis is an estrogen-dependent condition. Estradiol concentration greater than 60pg/ml
- 20. Increased concentration of macrophages derived growth factors including vascular endothelial growth
- 21. Sign &Symptoms SIGNS Tenderness in cul-de-sac Nodularity in cul-de-sac Fixed retroverted
- 22. Clinical Features Symptoms: Pelvic- Dysmenorrhea(50%) Abnormal menstruation(60%)
- 23. Dysmenorrhea Most common symptom Pain starts a few days prior to
- 24. Dyspareunia It is usually deep, due to stretching of the structures
- 25. Infertility Present in majority of the women with endometriosis. Advanced disease,
- 26. Diagnosis Recommended that pelvic examination be performed at the time of
- 27. Bimanual Pelvic Examination Examination On bimanual pelvic examination, fixed retroverted uterus,
- 28. Classification
- 30. Diagnosis Investigations Laparoscopy: Gold standard It should not be performed within
- 31. Diagnosis MRI
- 32. Diagnosis Histological Confirmation: Visual inspection is usually adequate but histological confirmation
- 34. Diagnosis Laparoscopy (Sensitivity : 97%, Specificity 95%) Types of lesions on
- 37. LAPROSCOPIC IMAGES : A )OLD ENDOMETRIOSIS (Blue/Grey) B ) OLD ENDOMETRIOSIS (Red)
- 38. Tranvaginal Ultrasound scan Retroverted uterus with obliteration of cul-de-sac & B\L
- 40. CA-125 Increased in moderate to severe endometriosis Also increased in non-mucinous
- 41. Extensive Pelvic Endometriosis
- 42. Dense Adhesions
- 43. Diagnosis Sonographic Features : Endometritic cysts (oval or round)- capsulated, fine
- 44. Differential Diagnosis Chronic PID Postoperative adhesions Old ectopic gestation Pelvic
- 46. Drug Treatment Combined oral contraceptives: Administered intermittently or continuously. High
- 47. Drug Treatment Danazol A synthetic derivative of ethinyl testosterone, Mildly
- 48. Drug Treatment Gonadotropin releasing hormone: GnRH is administered continuously to
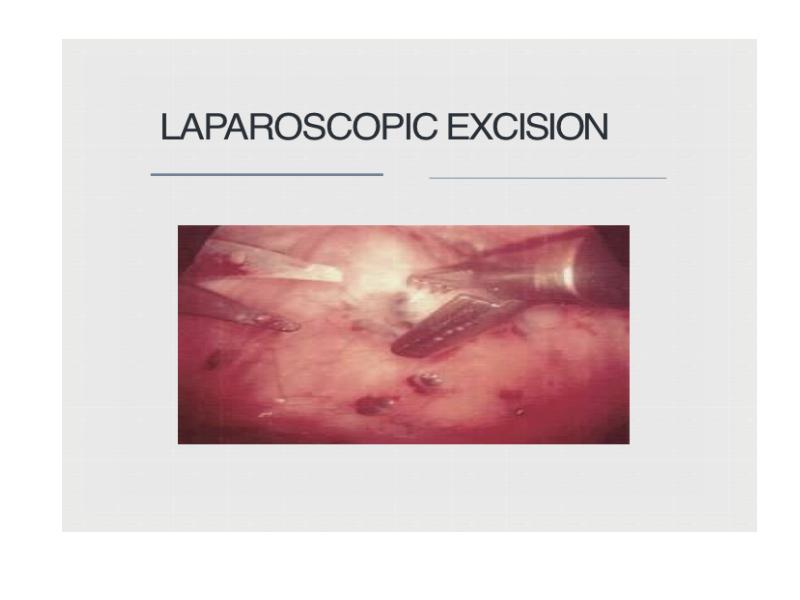
- 49. Minimal Invasive Surgery Aspiration of peritoneal fluid in cul-de-sac. Destruction of
- 50. Minimal Invasive Surgery Role of surgery: u Failed Medical therapy
- 53. Surgery Indications for surgery: Advanced stage of disease detected Large lesion
- 54. Surgery Laparotomy: In advanced & larger lesions if medical therapy
- 55. Combined Therapy Preoperative GnRH: monthly for 3 months reduces size
- 56. Prophylaxis Low-dose OCP reduce the menstrual flow & protect against endometriosis.
- 57. THANK YOU
- 58. Скачать презентацию





 - between the menarche and")

Metaplasia of coelomic epithelium")

John Sampson first postulated that endometriosis")

In this theory, the germinal epithelia")

Endometrial cell can be transported to")







")









 Types of lesions on")

OLD ENDOMETRIOSIS (Blue/Grey) B ) OLD ENDOMETRIOSIS (Red)")





- capsulated, fine")












Слайды и текст этой презентации
Слайд 1
Описание слайда:
ENDOMETRIOSIS
By
Dabiang & Tneki
153A - LA1
Teacher- Kamilova I.K
Слайд 2
Описание слайда:
ENDOMETRIOSIS
INTRODUCTION OF ENDOMETRIOSIS
SITES
AETIOLOGY
THEORIES FOR ENDOMETRIOSIS
CLINICAL FEATURES
CLASSIFIC ATION OF ENDOMETRIOSIS
PATHO-PHYSIOLOGY
DIAGNOSIS OF ENDOMETRIOSIS
MANAGEMENT
Слайд 3
Описание слайда:
Слайд 4
Описание слайда:
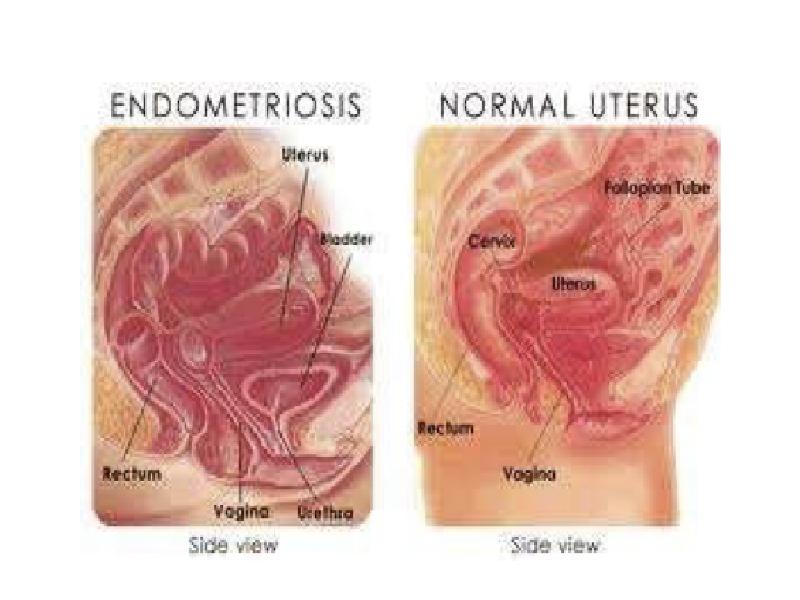
INTRODUCTION
Endometriosis initially described by Von Rokitansky in 1860
Endometriosis is a clinical and pathological entity.
It is characterized by the presence of tissue resembling functional endometrial glands and stroma outside the uterine cavity.
It is not a neoplastic condition, but malignant transformation is possible.
Слайд 5
Описание слайда:
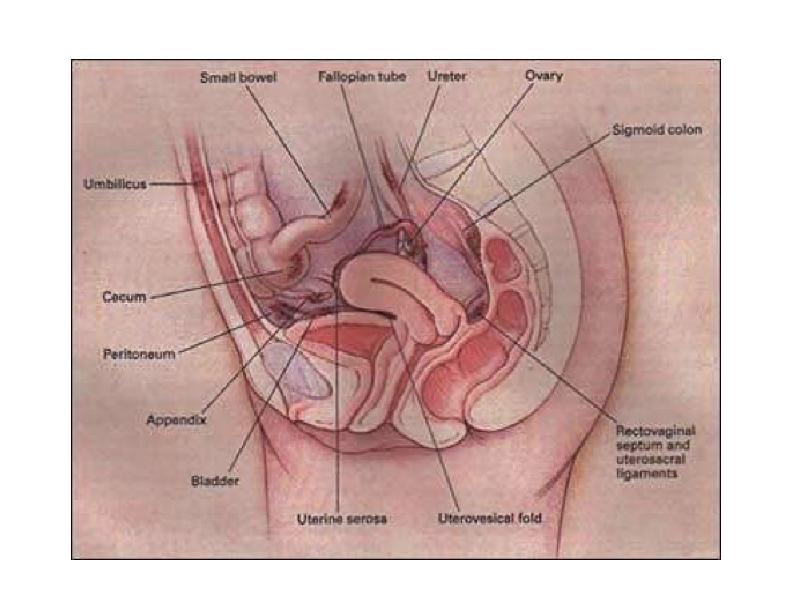
SITES
ABDOMINAL
Most common site - OVARY (44% involved)
Pouch of Douglas
Uterosacral ligament
Broad ligament
Rectovaginal septum
Pelvic lymph node
Rare sites - Gut, Appendix, Ureter, Urinary Bladder
Слайд 6
Описание слайда:
Слайд 7
Описание слайда:
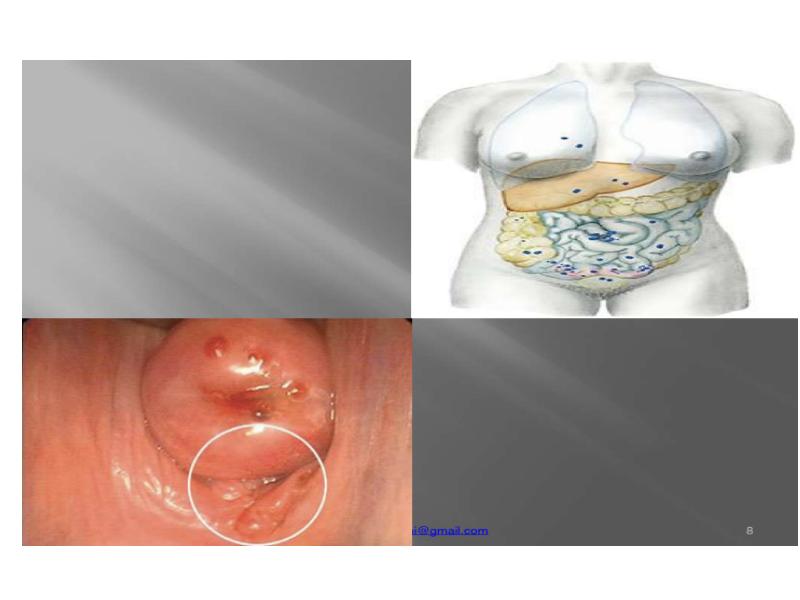
EXTRA-ABDOMINAL
EXTRA-ABDOMINAL
Common sites - Abdominal scar of Hysterotomy,
Caesarean Section,
Tubectomy,
Myomectomy
Umbilicus
Episiotomy Scar
Vagina
Cervix
Remote sites - Pleura, Lungs, deep tissues of arms, thighs
Слайд 8
Описание слайда:
Слайд 9
Описание слайда:
AETIOLOGY
Age - 30-40 years(most common) - between the menarche and menopause.
Family history - 7 times greater if 1st degeneration affected by endometriosis.
New study - Early menarche
Social and Economic factors - more common in highly civilized communitis .
Parity- 50-70% affected women are childless.
Слайд 10
Описание слайда:
Theories for Endometriosis
Retrograde menstruation (Sampson’s theory)
Metaplasia of coelomic epithelium (Meyer and Ivanoff)
Lymphatic dissemination
Haematogenous Spread
Hereditary factor
Immunologic factor
Induction theory
Слайд 11
Описание слайда:
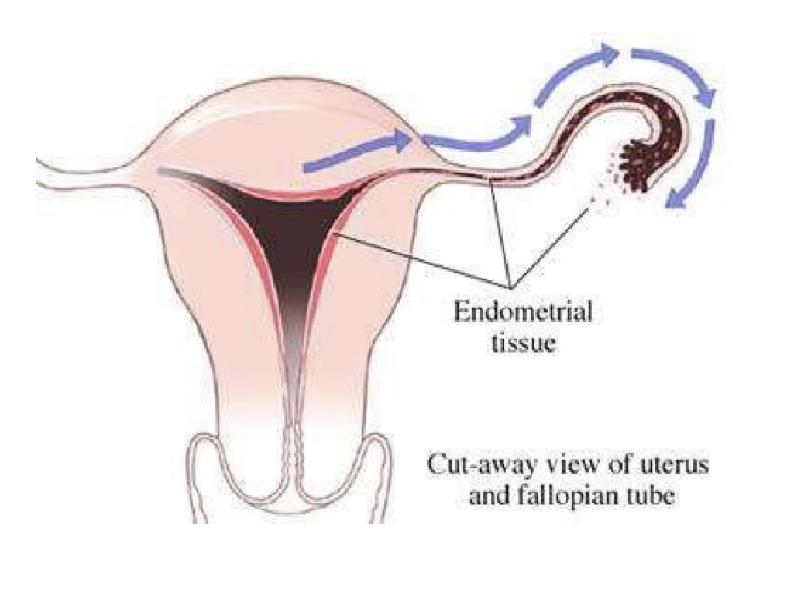
Retrograde menstruation ( Samson’s Theory)
John Sampson first postulated that endometriosis arose from retrograde flow of fragments of endometrial tissue through the oviducts and into the peritoneal cavity.
Epidemiologic data suggests that women who menstruate more frequently, more heavily, or for a longer duration have increased chance of disease development.
There is retrograde flow of menstrual blood through the uterine tube during menstruation. The endometrial fragments get implanted in the peritoneal surface of pelvic organs( Sites– ovaries, uterosacral ligament)
Anomalies of the Mullerian tract, increased occurrence of endometriosis and stenosis of external cervical os.
Слайд 12
Описание слайда:
Слайд 13
Описание слайда:
Coelemic metaplasia( Mayer And Ivanol)
In this theory, the germinal epithelia of the ovary, endometrium and peritoneum all originate from the same totipotential coelomic epithelium.
In coelomic Metaplasia, these totipotential coelomic cell are transformed by repeated exposure to hormonal or infection stimuli.
Development of endometriotic lesions in unusual locations.
Prolonged treatment with estrogen.
Слайд 14
Описание слайда:
Lymphatic Theory (vascular theory )
Endometrial cell can be transported to extrauterine sites by blood vessels or the lymphatic system or by contamination of the pelvis or abdominal wall incision, if the uterine cavity is surgically entered.
Слайд 15
Описание слайда:
Genetic factors
The risk or endometriosis is 7 times greater if a first- degree relative has been affected by endometriosis .
Multifactorial inheritance has been postulated.
Monozygotic twins are markedly concordant for endometriosis.
A worldwide collaborative project (The Oxford Endometriosis Gene Study) has been organized to identify a genetic basis for endometriosis
Слайд 16
Описание слайда:
Autoimmune theory
In cellular immunity, can facilitate the successful implantation of translocated endometrial cells.
In endometriosis lymphocytes decreased cytotoxic response to endometrial cell may be due to defect in natural killer cell activity, such as a decreased lytic effect toward stroma that allow ectopic development of endometrial fragments.
There may be increased resistance of endometrium in women with endometriosis to natural killer cytotoxicity.
Слайд 17
Описание слайда:
Induction theory
The induction theory is, in principle, an extension of the coelomic metaplasia theory.
It proposes that an endogenous (undefined) biochemical factor can induce undifferentiated peritoneal cells to develop into endometrial tissue.
This theory has been supported by experiments in rabbitsbut has not been substantiated in women and primates.
Слайд 18
Описание слайда:
Inflamation
Substantial evidence suggests that endometriosis is associated with a state of subclinical peritoneal inflammation, marked by
↑ peritoneal fluid volume,
↑ peritoneal fluid white blood cell concentration
↑ inflammatory cytokines, growth factors, and angiogenesis-promoting substances
Macrophages or other cells may promote the growth of endometrial cells by secretion of growth and angiogenic factors such as epidermal growth factor (EGF)
There is increasing evidence that local inflammation and secretion of prostaglandins (PG) is related to differences in endometrial aromatase activity between women with and without endometriosis
Слайд 19
Описание слайда:
Pathophysiology
Endometriosis is an estrogen-dependent condition.
Estradiol concentration greater than 60pg/ml is necessary for proliferation of endometrial lesions.
Estrogen & Progesterone receptors are found in much lower concentrations in endometriotic tissue than in normal endometrial tissue,
Growth factors can originate from the peritoneal environment to stimulate endometrial development.
Platelet derived growth factor, macrophage secretory
products enhance endometrial stromal cell proliferation.
Слайд 20
Описание слайда:
Increased concentration of macrophages derived growth factors including vascular endothelial growth factor.
Increased concentration of macrophages derived growth factors including vascular endothelial growth factor.
Molecular alterations in steroidogenic enzyme function have been implicated in the pathogenesis of endometriosis.
Menstrual effluent contains factors that induce alterations in the peritoneal mesothelium, facilitating adhesions of endometrial cells.
Слайд 21
Описание слайда:
Sign &Symptoms
SIGNS
Tenderness in cul-de-sac
Nodularity in cul-de-sac
Fixed retroverted uterus
Adnexal tenderness
Adnexal masses
Слайд 22
Описание слайда:
Clinical Features
Symptoms:
Pelvic- Dysmenorrhea(50%)
Abnormal menstruation(60%)
Dyspareunia,chronic pelvic pain
Premenstrual Spotting
Gastrointestinal - Constipation,diarrhea, hematochezia, tenesmus.
Urinary complaint- Flank pain,back pain, abdominal pain,urgency frequency hematuria.
Pulmonary - Haemoptysis, pneumothorax
Infertility.
Слайд 23
Описание слайда:
Dysmenorrhea
Most common symptom
Pain starts a few days prior to menstruation, gets worse during menstruation( secondary dysmenorrhoea)
Pain due to Increased secretion of PGF2α, Thromboxane β2 from endometriotic tissue.
Abnormal Menstruation:
Menorrhagia is a predominant abnormality.
Polymennorhoea, premenstrual spotting also occur.
Слайд 24
Описание слайда:
Dyspareunia
It is usually deep, due to stretching of the structures of the Pouch of Douglas or direct contact tenderness found in endometriosis of rectovaginal septum or Pouch of Douglas and with fixed retroverted uterus.
Abdominal pain:
lower abdominal pain or backache
May be due to inflammation in peritoneal implants due to cystic bleeding
Irritation or invasion of nerve
Action of inflammatory cytokines released by the macrophages.
Слайд 25
Описание слайда:
Infertility
Present in majority of the women with endometriosis.
Advanced disease, adhesions and fixity results in structural damage to
tubes and ovaries à impairs tubo-ovarian mobility.
Ovarian problems: anovulation, luteinized unruptured follicle, oocyte maturation defects.
Tubal problem: altered tubal motility or ovum pick up.
Peritoneal factors: intraperitoneal inflammation
Sperm problems: phagocytosis by macrophages, inactivation by antibodies.
Endometrium: luteal phase defect, implantation defects
Слайд 26
Описание слайда:
Diagnosis
Recommended that pelvic examination be performed at the time of menses when tenderness is easier to detect.
The vulva, vagina, and cervix should be inspected for any signs of endometriosis, although the occurrence of endometriosis in these areas is rare (e.g., episiotomy scar).
The uterus is often in fixed retroversion, and the mobility of the ovaries and fallopian tubes is reduced.
Other possible signs of endometriosis include uterosacral or cul-de-sac nodularity, cervical displacement due to uterosacral scarring , painful swelling of the rectovaginal septum, and unilateral ovarian (cystic) enlargement.
Слайд 27
Описание слайда:
Bimanual Pelvic Examination
Examination
On bimanual pelvic examination, fixed retroverted uterus, bilateral pelvic tenderness, fixed or enlarged ovaries and painful uterosacral nodularity.
Deeply infiltrating nodules are most reliably detected when clinical examination is performed during menstruation. Adenomyotic uterus is seldom > 12 weeks, soft, smooth & tender in contrast to fibroid uterus. Isolated adenomyoma can be differentiated by presence of localised tenderness
Слайд 28
Описание слайда:
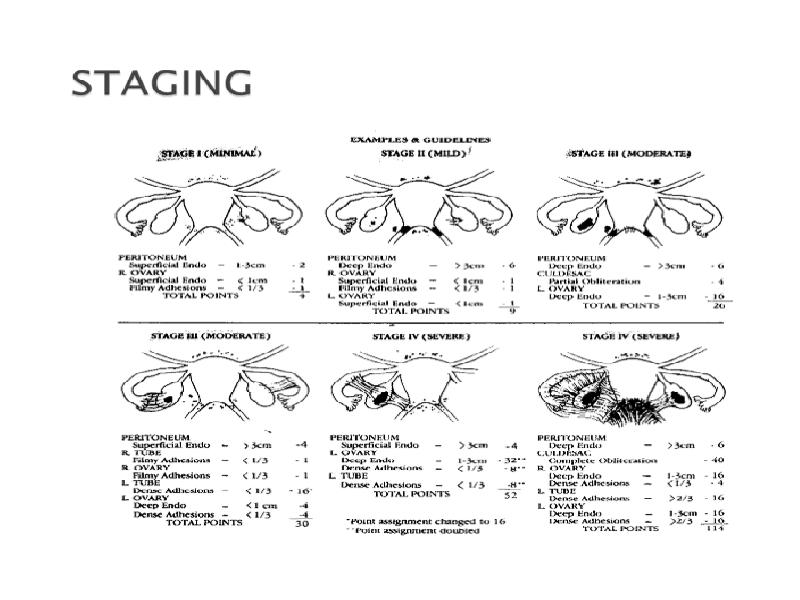
Classification
Слайд 29
Описание слайда:
Слайд 30
Описание слайда:
Diagnosis
Investigations
Laparoscopy: Gold standard It should not be performed within 3 months of hormonal treatment to prevent under diagnosis
Ultrasound: Ultrasound has a limited role, however the addition of colour doppler claims to increase the sensitivity to 91.8%, specificity of 91.3%
MRI –useful
Ca 125-Maybe elevated in severe
Слайд 31
Описание слайда:
Diagnosis
MRI
Слайд 32
Описание слайда:
Diagnosis
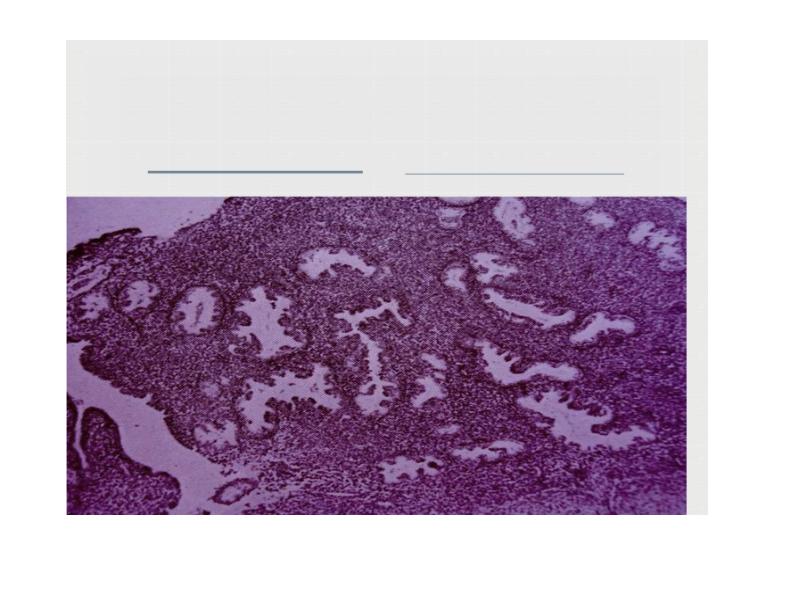
Histological Confirmation:
Visual inspection is usually adequate but histological confirmation of at least one lesion is ideal.
In cases of ovarian endometrioma >3 cm in diameter and in deeply infiltrating disease, histology is a must to rule out malignancy.
Слайд 33
Описание слайда:
Слайд 34
Описание слайда:
Diagnosis
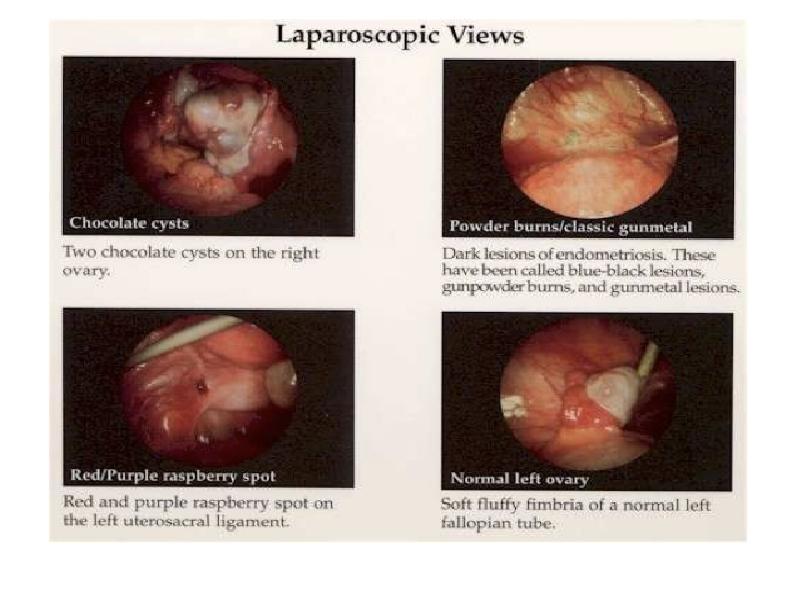
Laparoscopy (Sensitivity : 97%, Specificity 95%) Types of lesions on laparoscopy:
Powder burn or black lesions White opacified peritoneum Glandular excrescences Flame like red lesions
Peritoneal pockets or windows
Clear vesicles
Yellow brown patches
Unexplained adherence of ovary to peritoneum of ovarian fossa
Encysted collection of thick chocolate coloured or tarry fluids
Adhesions to posterior lip of broad ligaments/other pelvic structures
Слайд 35
Описание слайда:
Слайд 36
Описание слайда:
Слайд 37
Описание слайда:
LAPROSCOPIC IMAGES :
A )OLD ENDOMETRIOSIS (Blue/Grey) B ) OLD ENDOMETRIOSIS (Red)
C)OLD ENDOMETRIOSIS (Brown) D ) ACTIVE ENDOMETRIOSIS (Black)
Слайд 38
Описание слайда:
Tranvaginal Ultrasound scan
Retroverted uterus with obliteration of cul-de-sac & B\L complex adnexal masses maybe suggestive.
Helps to differentiate endometrial cysts from other complex cysts like dermoids:
Endometrial cyst: low level internal echoes with posterior acoustic enhancement – Ground glass appearance.
Dermoid: posterior acoustic shadowing d/t presence of bone & teeth in cyst. Presence of mural nodule & “pins and needle”.
Слайд 39
Описание слайда:
Слайд 40
Описание слайда:
CA-125
Increased in moderate to severe endometriosis
Also increased in non-mucinous epithelial ovarian cancers.
Слайд 41
Описание слайда:
Extensive Pelvic Endometriosis
Слайд 42
Описание слайда:
Dense Adhesions
Слайд 43
Описание слайда:
Diagnosis
Sonographic Features :
Endometritic cysts (oval or round)- capsulated, fine homogeneous, uniform, granular echoes, anechoic, single or multiple, unilateral or bilateral
On Doppler: no vascularity within the mass Ovarian adhesions to uterus
Free floating fimbria on sonosalpingography
Слайд 44
Описание слайда:
Differential Diagnosis
Chronic PID
Postoperative adhesions
Old ectopic gestation
Pelvic congestion syndrome
Irritable bowel syndrome
Diverticulitis
Ulcerative colitis
Crohn’s disease
Слайд 45
Описание слайда:
Слайд 46
Описание слайда:
Drug Treatment
Combined oral contraceptives:
Administered intermittently or continuously.
High Incidence of side effects & risk of thrombus-embolism limit their prolonged use.
Seasonal OC for 84 days , with 6 days tablet free, reduce the menstrual periods to just four cycles in a year.
Oral progestogens:
Exert an anti-oestrogenic effect and their continuous administration causes decidualization and endometrial atrophy.
Norethisterone 5.0 – 20.0mg daily or Dydrogesterone 10 -30mg daily.
This hormone does not prevent ovulation and is suitable for a woman
trying to conceive.
Слайд 47
Описание слайда:
Drug Treatment
Danazol
A synthetic derivative of ethinyl testosterone,
Mildly anabolic , anti-oestrogenic and anti-progestational
200-800mg daily for 3-6 months starting on first day of menses.
S/E: wt. gain, hirsutism, excessive sweating, muscle cramps,
depression, atrophy of breasts & vaginal epithelium.
Aromatase inhibitors:
Letrozole(2.5mg), anastrozole(1-2mg) daily for 6 months.
Anti-oestogenic & prevent conversion of androgen to oestrogen.
Should be given with Vitamin D and Calcium to prevent osteoporosis.
Nausea , vomiting and diarrhea are other side effects.
Слайд 48
Описание слайда:
Drug Treatment
Gonadotropin releasing hormone:
GnRH is administered continuously to down regulate and suppress pituitary gonadotropins .
It causes atrophy of endometriotic tissue.
The synthetic analogue of GnRH is given in doses of 10-20mg
intravenously twice daily.
Prolonged GnRH therapy over 6months causes hypo-oestrogenism & menopausal symptoms such as hot flushes, dry vagina, urethral syndrome and osteoporosis.
RU-486:
Tried at a dose of 50mg daily for 3months.
Reduces pain and delay recurrences.
Слайд 49
Описание слайда:
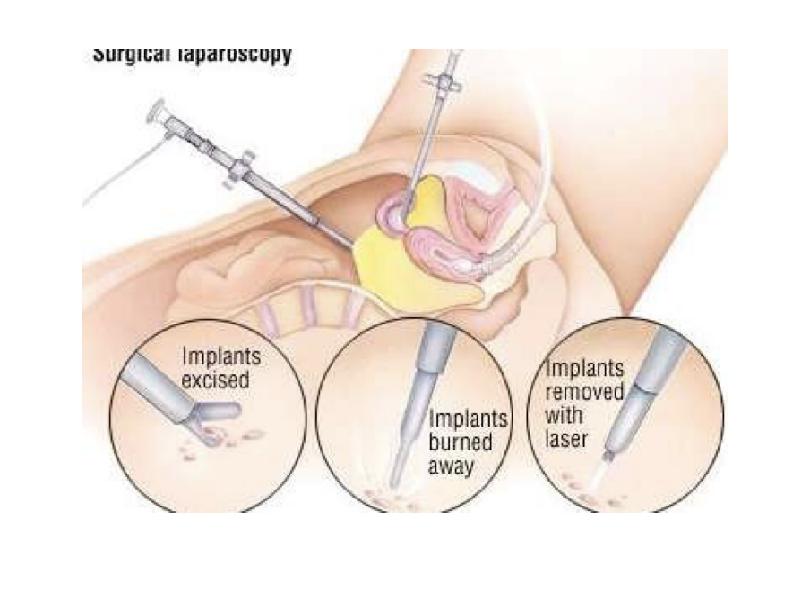
Minimal Invasive Surgery
Aspiration of peritoneal fluid in cul-de-sac.
Destruction of endometriotic implants <3cm by diathermy cauterization or vaporization by CO2 or Nd:YAG laser.
Larger lesions and chocolate cyst can be excised. Residual lesion can be dealt with by hormonal therapy. Cauterization of cyst wall – young females.
Слайд 50
Описание слайда:
Minimal Invasive Surgery
Role of surgery:
u Failed Medical therapy
u Infertility
u Recurrence
u Chocolate cyst ovary
Laparoscopic breaking of adhesions in pelvis relieves dysmenorrhea and pelvic pain.
LUNA (Laser uterosacral nerve ablation) for midline pain.
Prolapse of genital tract & bladder dysfunction is noted with LUNA.
Слайд 51
Описание слайда:
Слайд 52
Описание слайда:
Слайд 53
Описание слайда:
Surgery
Indications for surgery:
Advanced stage of disease detected
Large lesion
Medical therapy fails or intolerable
Recurrence occurs
In elderly parous women
Aim:
Coagulation of peritoneal endometrial lesions
Adhesiolysis
Fenestration & drainage of small ovarian endometriomas <3cm diameter. Cystectomy- >3cm.
Слайд 54
Описание слайда:
Surgery
Laparotomy:
In advanced & larger lesions if medical therapy fails.
Dissection and excision of a chocolate cyst.
Salpingo-oophorectomy
Abdominal hysterectomy and bilateral salpingo-oophorectomy.
Premenopausal woman may need HRT after radical surgery.
HRT following bilateral ovarian removal in young women may be prescribed under strict monitoring, as a risk for recurrence remains.
Total hysterectomy & B/L oophorectomy- women with severe
symptoms & those with fertility is not a problem.
Слайд 55
Описание слайда:
Combined Therapy
Preoperative GnRH:
monthly for 3 months
reduces size & extend of lesions,
softens adhesions
makes subsequent surgery more easier & complete.
Postoperative hormonal therapy:
When surgery is incomplete or some residual lesion is left behind.
Слайд 56
Описание слайда:
Prophylaxis
Low-dose OCP reduce the menstrual flow & protect against endometriosis. 3 monthly OCP’s are convenient to take & effective.
Tubal patency tests should be avoided in immediate premenstrual phase to avoid spill.
Operations on genital tract should be scheduled in postmenstrual period.
Слайд 57
Описание слайда:
THANK YOU
Скачать презентацию на тему ENDOMETRIOSIS можно ниже: